

Trigger choices
Gonadotropin releasing hormone agonist (GnRHa) trigger is more physiological than human chorionic gonadotropin (hCG) or Ovidrel trigger

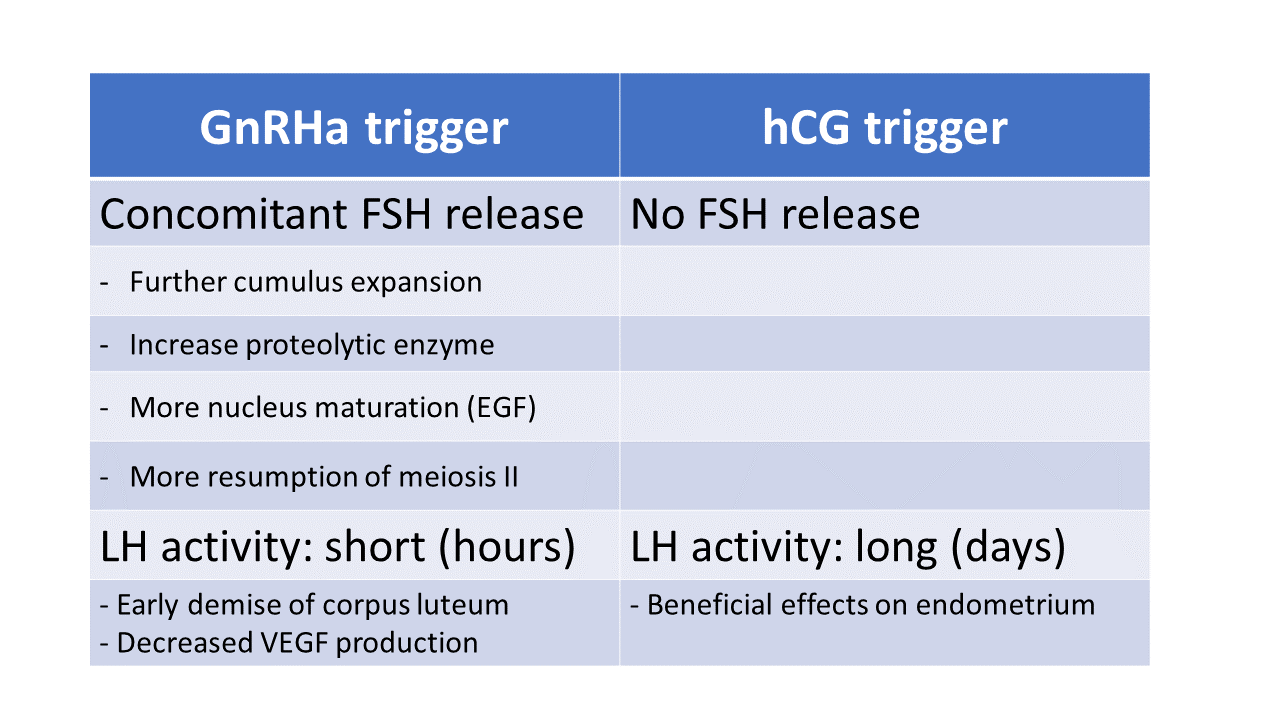
GnRHa trigger mimics natural LH surge in that both LH and FSH are released. It may be the solution to well-executed cycles that ended unexpectedly badly
Ms. Scott comes to discuss her next IVF cycle. She had 18 mature follicles but only 11 eggs were retrieved. Four of the nine mature eggs became fertilized. Three became blastocysts; one was confirmed euploid. She did not conceive after embryo transfer.
Ms. Scott received Gonal-f, Menopur and antagonist for ovulation induction. The trigger was 10,000 units hCG (human chorionic gonadotropin). The ovulation induction was considered satisfactory. So were the retrieval and transfer. I recommend keeping the same regimen for ovulation induction but changing trigger to Lupron 5 mg and hCG 3,300 units. Jennifer, one of our fellows, asks why.
Trigger shot initiates the final steps of oocyte maturation. Resumption of meiosis II and induction of proteolytic enzymes aiding the release of egg are well known functions of the trigger. Less well known is the concomitant rise of FSH, which increases LH receptors, may aid oocyte maturation, and other actions on the endometrium.
Anecdotal reports suggest GnRHa (Gonadotropin releasing hormones, such as Lupron) trigger may be the solution to “Empty follicle syndrome” and “Immature oocyte syndrome.” The former describes cases where the actual number of eggs retrieved is far below the expectation based on the number of mature follicles. The latter, the percentage of immature oocytes is > 25% of oocyte retrieved in a well-executed cycle. Despite solid studies are lacking, GnRHa trigger appears to be a logical choice, because it is more physiological than sole hCG (or Ovidrel, a recombinant hCG) trigger.
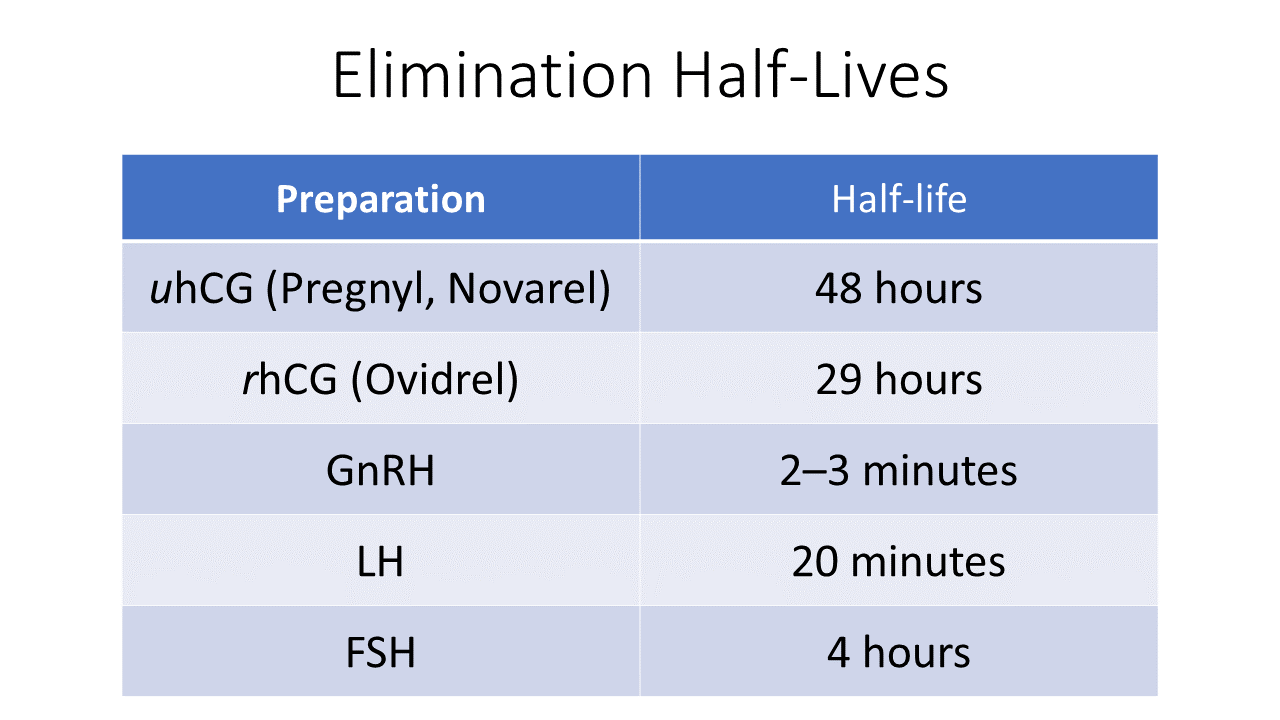
Due to the short half-life of LH (relative to hCG), studies showed fresh IVF cycles using GnRHa trigger requires luteal support, such as Progesterone (50 mg IM daily) and Estrogen (three 0.1mg patches every two days) or small doses of hCG (mostly used in Europe). In IVF + PGT (Pre-implantation Genetic Testing) cycles, no supplement is needed. However, as insurance against individuals with LH receptor variants (requiring longer exposure to LH), a small dose of hCG (or Ovidrel) is added. This is the so-called “dual trigger.”
GnRHa trigger can be achieved by Lupron (mostly used in US), Buserelin 0.5 mg or Triptorelin 0.2 mg (mostly used in Europe). The reported doses of Lupron vary from 1 mg, 2 mg to 5 mg. For dual trigger, both hCG or Ovidrel in various doses can be used.
In Ms. Scott’s case, I suggest a dual GnRHa trigger: Lupron 5 mg + 3,300 units hCG. No supplement is needed as this is a IVF + PGT cycle.