The Vecchietti procedure and Mayer-Rokitansky-Küster-Hauser Syndrome
Dilatation, self or through the Vecchietti procedure (in my opinion) is most convenient for patients with Mayer-Rokitansky-Küster-Hauser Syndrome.

Once self dilatation fails, patients are faced with different surgical choices. In my opinion, the Vecchietti procedure is the least intrusive, because it is essentially a method of active dilatation. The surgery (a laparoscopy) is performed to place the device.
Three-step approach to Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome
MRKH syndrome has a prevalence of 1 in every 5,000 - 7,000 girls. Its diagnosis and managements are discussed in my 8/11/2024 post (“Mayer-Rokitansky-Küster-Hauser Syndrome: 3-step approach”).
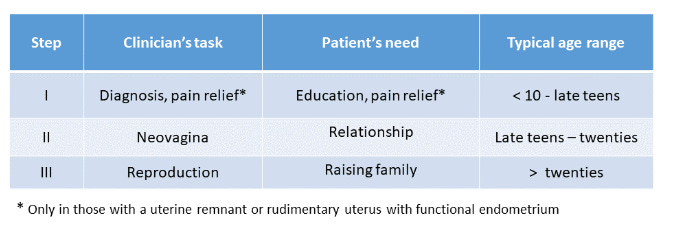
Management of girls with MRKH can be divided into three steps. Patients have different needs in each step; clinicians have different tasks. They are summarized in the table below.
Neo-vagina creation
Many methods have been described to create a neovagina. Based on the driving force that creates the vagina, they can be grouped into non-surgical and surgical method.
Non-surgical method: manual dilatation, Frank’s bicycle, and Vecchietti procedure.
Surgical method: McIndoe Procedure (mainly in the US), Davydov Procedure, Williams Vaginoplasty, Amniotic Membrane, Wharton-Sheares-George method, and intestinal (bowel) vaginoplasty, which uses a segment of ileum or colon to create neo-vagina.
Vecchietti procedure belongs to non-surgical method, because surgery is used to place the traction device; it is pulling of the olive (active dilatation) that creates the neo-vagina.
The original Vecchietti procedure
The Vecchietti procedure was first described by Dr. Giuseppe Vecchietti in 1965 (Attual Ostet Ginocol 1965;11:131-47). Later, he reported 307 consecutive cases in 1979 and 1980. Dr. Vecchietti performed laparotomies to place the traction devices.
The first modification of the original Vecchietti procedure was reported in 1994 (Am J Obstet Gynecol 1994;171 :268-9). The authors used laparoscopy to guide the Vecchietti needle.
Instrument used in Vecchietti procedure
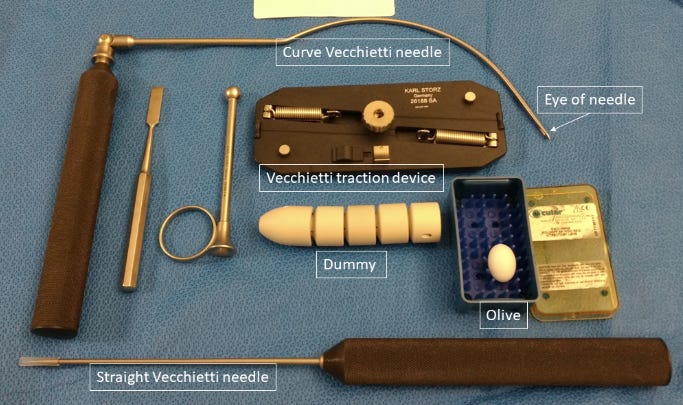
Figure below shows the instrument used in Vecchietti procedure. Traction device has evolved over time. Earlier version is made by stainless steel with spring on each side. The tension of the thread (suture) pulling the olive is controlled by two nuts. Newer version uses one dial to control the spring tension. Once the dial is turned, both springs tightened simultaneously, ensuring equal pull on the olive.
Laparoscopy-assisted Vecchietti procedure
Figures and steps of a laparoscopy assisted Vecchietti procedure first described in 1994 are summarized below.
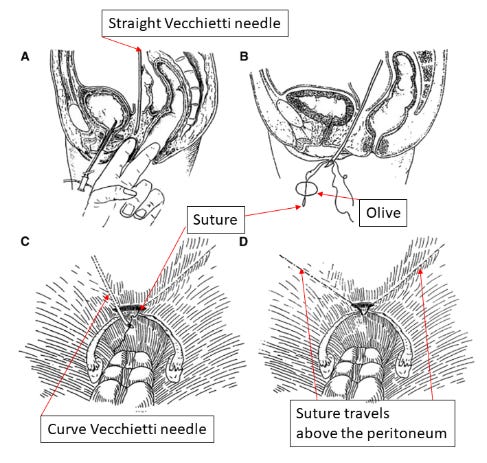
The straight Vecchietti needle is advanced through the vesico-rectal space with concomitant laparoscopy and cystoscopy.
The tip of the straight needle meets and the tip of operator’s index finger pushing upwards (also in the vesico-rectal space). The operator’s middle finger is in the rectum, guiding the needle downwards.
The needle exits from the would-be vaginal opening.
A suture (thread) passes through the eye of an Olive and hooked to the straight needle.
Needle is then pulled back to the peritoneal cavity, bring both ends of the suture with it.
One end of the suture is hooked to the curve Vecchietti needle, which enters via an accessory port, travels above the peritoneum and exits where the suture enters the pelvis.
Pulling curve Vecchietti needle out of the accessory port will bring the suture above the peritoneum and exit through the accessory port.
Suture is then hooked up with the traction device. The spring of the device pulls the olive cephalad (upwards). This is active dilatation.
The spring is tightened daily, usually advancing 1.5 - 2 cm daily.
When vaginal length is 7.5 - 10 cm (usually takes about 5 days), the string is cut, the olive and the traction device are removed.
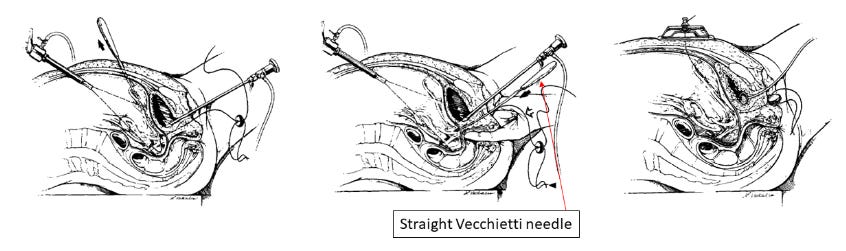
A modification of the above method has been reported (figure below). It involves reversing the direction of the straight Vecchietti needle: the needle (with two ends of a suture) is advanced upwards to the pelvis from the would-be location of the vagina opening. The operator’s index or middle finger is placed in the rectum.
Some pertinent facts about Vecchietti procedure
Below are pertinent facts about Vecchietti procedure:
The surgical procedure to place the device takes about one hour.
The treatment (active dilatation) begins after the surgery is over.
Some providers keep patients in the hospital; some discharge them
If hospitalized, patients usually have continuous epidural or PCA.
The dial is tightened so that the suture (thread) is pulled upwards 1.5 - 2 cm daily. This is done at bed side or in the clinic.
A 7.5 -10 cm vagina is usually attained in 5 days.
Continuous dilatation (or vaginal intercourse) is needed to maintain the length of the vagina.
=====
To dear readers,
Access to “Fertilityandhormones” will become partially subscription-based in the near future. Some posts will remain free, but others (including archives) will be accessible to subscribers only.
Income will be used to defray the preparation costs. Furthermore, the number of subscribers shows the extent to which readers value “Fertilityandhormones”.
Thank you!
Dr. Huang
Thank you for the comment. Knowledge gap prevents access to treatment - patients and physicians alike.
(1) Could you please share the information with who you know? They may know someone who needs help.
(2) If you are interested in becoming an advocate of RKH, I know someone in Texas Children's Hospital, who is passionate about RKH education.
Thank you.
Dr. Huang
As someone who has MRKH and wanted more information on the surgery, your post was super helpful!!!