
Early pregnancy bleeding
Early pregnancy bleeding
Bleeding is common during the first three months of pregnancy. Most of the subchorionic hematoma is harmless.

Ms. Simpson is pregnant after having a frozen embryo transfer (FET). She is in the clinic because she has been having vaginal bleeding since yesterday. She denies pelvic cramps. A transvaginal ultrasound four days prior showed a normal pregnancy of 6 weeks and 3 days. Today’s ultrasound confirms the on-going pregnancy and a 22 x 15 x 13 mm space between the uterus and the placenta. Ms. Simpson is concerned.
Vaginal bleeding during the first 12 weeks of pregnancy is common. One survey revealed one in three new mothers recall such bleeding. The real number is likely to be higher. Either cervix or uterus may be the source of bleeding. A speculum inspection can differentiate the two. By comparison, cervix is far less likely to be the cause of bleeding.
Bleeding from the cervix may occur spontaneously or after intercourse. It may be due to new growth (such as cervical cancer or cervical polyp) or changes due to hormones (such as cervical erosion or congested/fragile cervix).
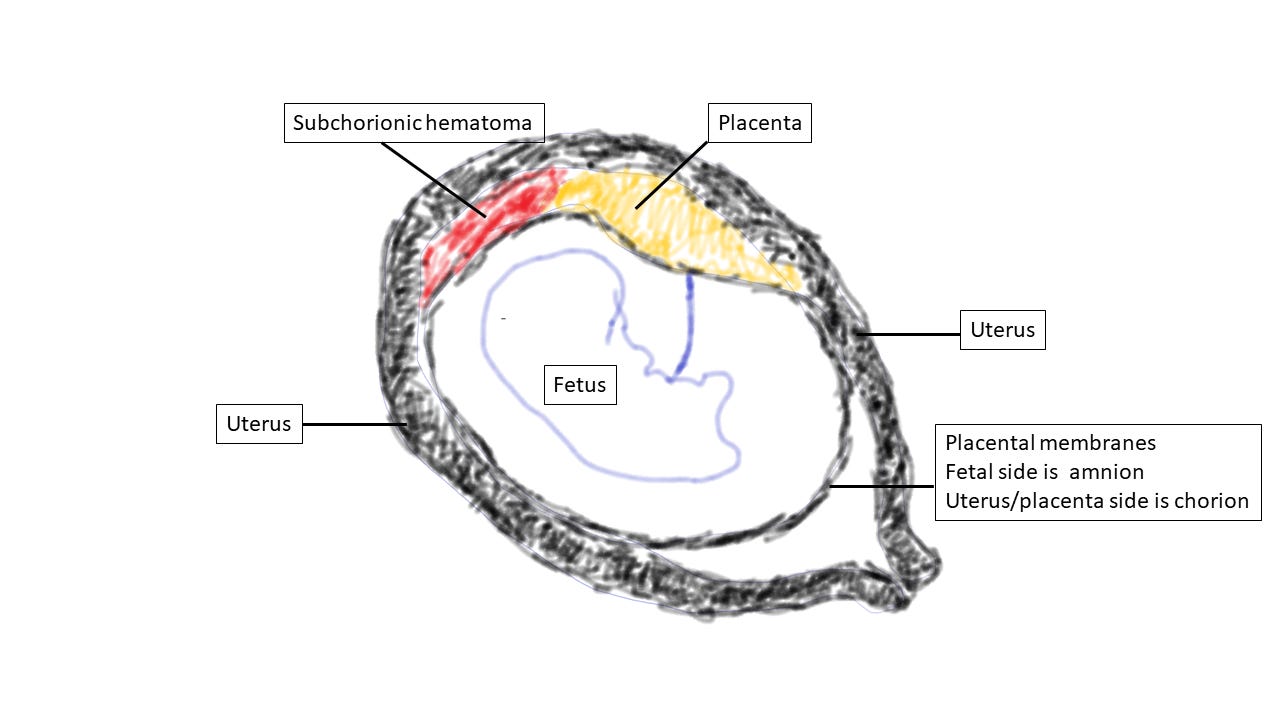
Bleeding from the uterus (i.e., the pregnancy) may be due to (1) a failed pregnancy (an on-going miscarriage), (2) a failing pregnancy (an on-going pregnancy eventually leads to a miscarriage), or (3) an on-going pregnancy which has a “subchorionic hematoma”, a blood clot between the chorion and the uterus.
The chorion is one of the placental membranes that attaches the amnion, the other placental membrane holding the amniotic fluid, to the uterus. Contrary to most people’s belief, few people have miscarriage because they have low progesterone. Low progesterone is the result of a failing pregnancy (I will explain in a separate article).
Chromosomes hold genetic codes, which guide the development of an embryo (early fetus). Chromosome analysis showed more than 75% of miscarriages have abnormal chromosomes – the number of chromosomes is not 46. Thus, failed pregnancies or failing pregnancies mentioned above fall into this category.
The cause of subchorionic hematoma is unknown. One possible explanation is blood vessels of the placenta are torn by a shear force generated by the “mismatch” between the growth of the uterus and the placenta. Blood escapes between the chorion and the uterus, creating a space. If this space is connected with the cervical canal, blood exits to the vagina. Otherwise, the hematoma is usually an incidental finding during a routine ultrasound exam.
Serial ultrasound observation is the management for subchorionic hematoma. Luckily, most of the time the bleeding decreases, the hematoma shrinks, and the pregnancy progresses. Rarely, bleeding increases and/or the hematoma enlarges leading to miscarriage. I ask patients to seek urgent medical attention (to find out what is happening) if the bleeding is more than the heaviest day of menstruation.
I explained to Ms. Simpson the natural course of subchorionic hematoma. I asked her to have pelvic rest and return in one week for another ultrasound. I also inform her to seek medical care urgently if the bleeding is heavier than the heaviest day of her menstruation,